Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
📄 Free 2-Week Rehab Program — request your copy
What Is Patellar Tendinopathy?
The patellar tendon connects the inferior pole of the patella to the tibial tuberosity. It is the distal component of the knee extensor mechanism — receiving the force generated by the quadriceps through the patella and transmitting it to the tibia to extend the knee. In activities that require rapid energy storage and release — jumping, landing, sprinting, change of direction — the patellar tendon functions as a spring, absorbing and returning elastic energy with each loading cycle. It is this energy-storage function that distinguishes patellar tendinopathy from other anterior knee conditions and that drives both the presentation and the rehabilitation approach.
The hallmark of patellar tendinopathy is pain localised to the inferior pole of the patella that is load-related — it increases specifically with activities that demand energy storage from the knee extensor mechanism. The condition warms up during activity (unlike patellofemoral pain, which typically worsens through activity), and it flares in the 24 hours after excessive loading [134]. This 24-hour response window is clinically important: pain that settles within 24 hours of an activity indicates an acceptable load; pain that persists beyond 24 hours indicates the tendon's capacity was exceeded.
The pathology is not inflammatory. Like all tendinopathies, patellar tendon pain reflects a degenerative and dysrepair process — disorganised collagen, altered matrix, and abnormal neovascularisation — rather than acute inflammation [126]. This explains why anti-inflammatory injections and NSAIDs provide only temporary relief: they target a process that is not driving the condition.
Presentation overview
| Feature | Detail |
|---|---|
| Pain location | Inferior pole of patella; well-localised; point-tender on direct palpation |
| Symptom pattern | Warms up during activity; flares 24 hours post-load; stiff at start of activity after rest |
| Provocative activities | Jumping, landing, sprinting, heavy squatting, decline walking |
| Differentiating feature | Warms up during activity (vs PFP which worsens); highly load-specific |
| Key clinical test | Single-leg decline squat — most sensitive provocative test for inferior pole pain |
| Most affected | Jumping athletes (volleyball, basketball, netball), heavy gym users, runners at high volume |
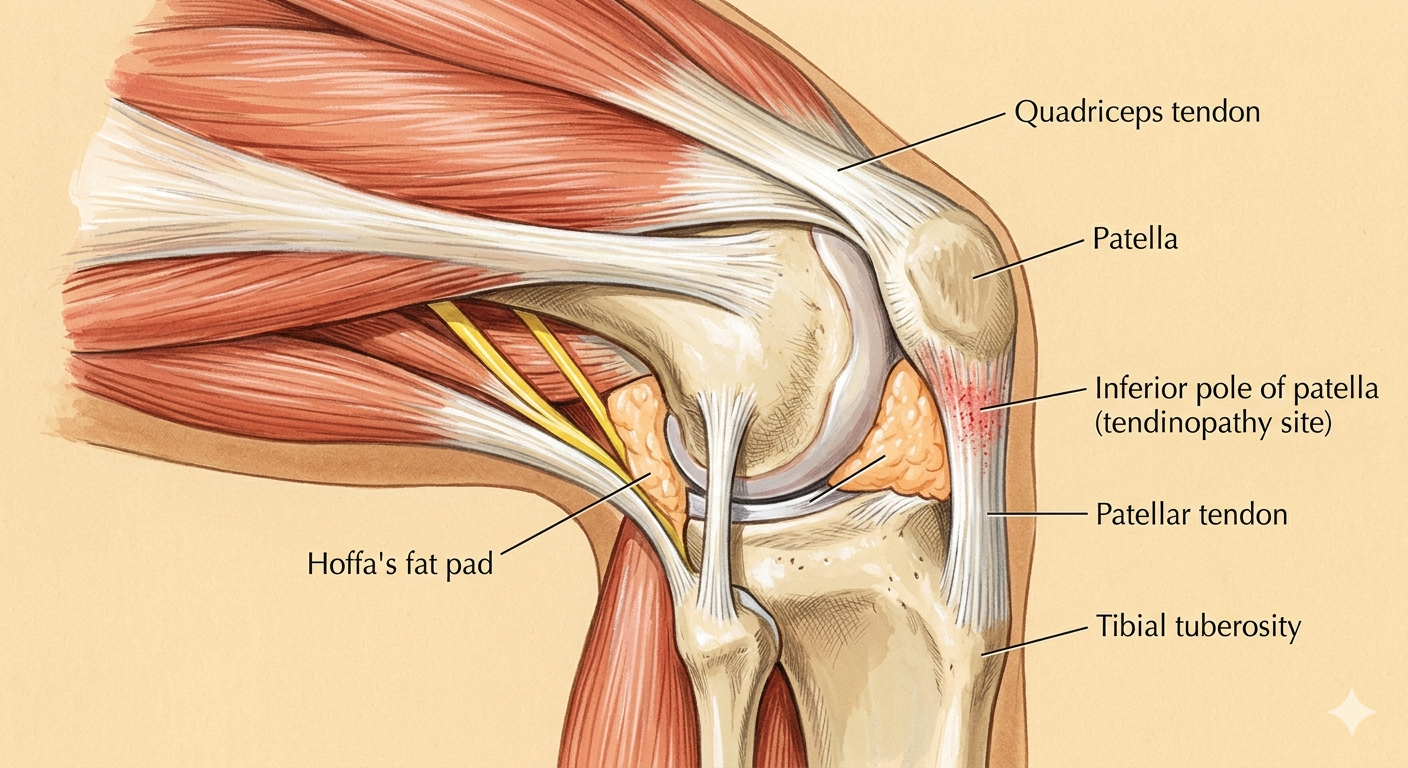
The knee joint — patella, patellar tendon, femoral condyles, and tibial plateau. The relationship between these structures, and the forces transmitted through them during movement, determines how load is distributed across the joint.
Who Typically Experiences This?
Jumping athletes
Volleyball, basketball, netball, and AFL players are the highest-prevalence group for patellar tendinopathy — so consistently that the condition is commonly called "jumper's knee." The combination of high-volume repetitive energy-storage loading in training and competition, with inadequate recovery and progressive strengthening to match the demand, creates the conditions for tendon dysrepair. In elite volleyball, prevalence rates exceed 40%. The Chelsea Heights and south-east Melbourne area has a large netball, basketball, and volleyball community in the 15–35 age bracket that represents this group.
Heavy gym users
High-volume squatting, leg press, and split squat work creates significant energy-storage demand on the patellar tendon, particularly at depth. Gym-goers who train lower limb heavy more than three times per week without adequate recovery, or who return to heavy lower-limb training after a deload period without ramping appropriately, are at elevated risk. The "reactive tendinopathy" stage — early, reversible — is the most common presentation in this group, and it is highly responsive to load management.
Runners at high volume
While patellar tendinopathy is less common than Achilles tendinopathy or patellofemoral pain in runners, it occurs in high-mileage runners and those who include significant hill or sprint work. The energy-storage demands of faster pacing and uphill/downhill running increase the load on the patellar tendon relative to easy flat running.
The in-season athlete who cannot stop
Patellar tendinopathy in active competition is one of the more challenging clinical scenarios. The athlete cannot fully offload the tendon, the loading continues through the season, and the tendon progressively moves along the degenerative spectrum. In-season management — reducing training load where possible, isometric loading for analgesia, protecting the tendon from reactive spikes — is a recognised clinical approach, but it requires specific management distinct from the rehabilitation approach used in the off-season [134].
The person returning to jumping or heavy loading after rest
A period of rest — whether from injury, illness, or a planned break — reduces the tendon's load tolerance. Returning to full training volume immediately exposes a deloaded tendon to loads it is no longer adapted to handle. Reactive tendinopathy is a common consequence, and it is the most reversible stage if identified and managed early [126, 134].
The Fascial Lens: Why We See This Differently
The patellar tendon is an energy-storage structure — the chain must absorb its share
The patellar tendon does not generate load. It transmits and stores the energy generated by the quadriceps and absorbed by the lower limb during impact activities. The total load the patellar tendon must handle is determined by how much of the impact energy the rest of the lower limb chain absorbs. When the hip extensors are insufficient, when ankle dorsiflexion is restricted, or when the calf-Achilles complex is underloaded, the knee — and specifically the patellar tendon — absorbs a disproportionate share of the energy storage demand with every landing and every loaded squat.
This is the kinetic chain argument for patellar tendinopathy: addressing the tendon in isolation, without assessing and rehabilitating the chain that determines its load, leaves the underlying driver in place. Hip mechanics, specifically, have a direct bearing on the loading pattern of the knee extensor mechanism [132]. When the hip extensors are contributing inadequately to the energy absorption of landing, the quadriceps-patellar tendon unit compensates.
The paratenon is a fascial structure
The patellar tendon is surrounded by a paratenon — a thin fascial sheath that allows the tendon to glide within its surrounding connective tissue. Like all fascial sheaths, the paratenon is subject to densification — particularly following periods of high compressive load or after a reactive episode. When the paratenon densifies, the tendon's gliding environment is compromised, contributing to the friction and load concentration at the inferior pole. This fascial component is distinct from the tendon pathology itself and is a target for Fascial Manipulation directed at the anterior knee region.
Tendinopathy as a continuum — the stage determines the approach
Cook and Purdam's tendinopathy continuum model identifies three stages with distinct tissue characteristics and management implications [126]:
- Reactive tendinopathy — a short-term proliferative response to acute overload. Reversible. Non-inflammatory. The primary management is load reduction to below the reactive threshold, then graduated reloading.
- Tendon dysrepair — matrix disorganisation, increased neovascularisation. Partially reversible. Progressive loading is the primary driver of remodelling.
- Degenerative tendinopathy — cell death, irreversible structural change in some regions. The goal of loading shifts from promoting remodelling to improving the function of the remaining healthy tissue.
Where the patellar tendon sits on this spectrum determines the entry point of the rehabilitation programme. A reactive tendon in a gym athlete after a heavy week is managed very differently from a chronically degenerated tendon in a long-term jumping athlete. Identifying the stage — through the symptom pattern, the 24-hour response, and the history of loading — is the first clinical task.
Isometric loading as an entry point
The evidence for isometric quadriceps loading as the initial stage of patellar tendinopathy rehabilitation is compelling. Isometric exercises — holding a wall sit or leg press position under load for 45-second holds at 70% maximal voluntary contraction — have been shown to reduce tendon pain immediately and to address the cortical inhibition that accompanies painful tendon loading. This provides an entry point for loading that does not expose the tendon to the energy-storage demand it cannot yet tolerate, while maintaining quadriceps load and volume [134].
What Does the Research Say?
The tendon must be progressively loaded — not rested
Clinical management of patellar tendinopathy should focus on progressively developing the load tolerance of the tendon, the musculoskeletal unit, and the kinetic chain, as well as addressing biomechanical risk factors. Rest does not resolve patellar tendinopathy; it temporarily reduces symptoms while allowing the tendon's capacity to decline further, setting up a reactive spike on return to activity [134].
A four-stage loading protocol — calibrated to tendon irritability
A clinical framework from La Trobe University (Melbourne) describes four rehabilitation stages: (1) isometric loading for analgesia and cortical drive; (2) heavy slow resistance — 3–4 sets progressing from 15RM to 6RM, every second day; (3) energy-storage loading (progressive jumping and plyometrics, every third day); (4) return to sport. Heavy slow resistance training was associated with 70% patient satisfaction compared to 22% for decline squat training at 12-month follow-up [134].
The 24-hour rule guides load progression
Pain that settles within 24 hours of a loading session indicates acceptable load. Pain persisting beyond 24 hours indicates the load ceiling was exceeded. This simple monitor provides a practical, patient-led tool for calibrating training load during rehabilitation — reducing the need to rely on symptom monitoring during the session itself, when the tendon typically warms up and the true load response is masked [134].
Tendinopathy is a continuum — stage determines management
The tendinopathy continuum model describes a spectrum from reactive (reversible, non-inflammatory) through dysrepair to degenerative change. The management at each stage differs. Load management is the primary intervention across the continuum, but the type of loading, the volume, and the recovery interval are stage-specific [126].
Hip mechanics contribute to patellar tendon load
Research on hip mechanics and knee injury establishes that inadequate proximal hip extensor and abductor function increases the load absorbed by the quadriceps-patellar tendon unit during impact activities. Addressing the hip and kinetic chain is a component of complete patellar tendinopathy rehabilitation [132].
How We Approach Patellar Tendinopathy
Stage identification and load assessment
Our assessment establishes where on the tendinopathy continuum the presentation sits — using the symptom pattern, 24-hour response, single-leg decline squat, and loading history. This determines the entry point for rehabilitation and the pace of progression [126, 134].
Fascial Manipulation assessment
We assess the anterior knee — the paratenon, infrapatellar fat pad, and anterior knee fascial system — for densification contributing to the tendon's mechanical environment. Using the Stecco FM approach, treatment at identified centres of coordination aims to restore the gliding capacity of the fascial sheath around the tendon [19].
Progressive tendon loading programme
We implement the four-stage loading framework calibrated to the current tendon irritability and monitored by the 24-hour response rule. We begin with isometric loading, advance through heavy slow resistance to energy-storage work, and progress to sport-specific loading at the pace the tendon's response guides [134].
Kinetic chain assessment and rehabilitation
We assess hip extensor strength, ankle dorsiflexion range, and the calf-Achilles complex. Where the chain is contributing to patellar tendon overload through insufficient energy absorption elsewhere, these components are incorporated into the rehabilitation programme [132].
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Use the 24-hour rule to monitor your load
After any lower-limb loading session, assess your tendon pain the following morning. If it has settled to your baseline level or better — the load was acceptable. If it is worse than baseline 24 hours later — the load was too much. This simple rule gives you a practical guide for adjusting training volume and intensity while rehabilitation progresses.
2. Start isometric loading
A wall sit held for 45 seconds, five repetitions, performed two to three times per day, is a simple and well-supported starting point for patellar tendinopathy rehabilitation. It loads the quadriceps without the energy-storage demand that provokes the tendon at its current irritability level. It also provides immediate analgesia in many presentations — making it useful before training or activity to reduce in-session pain.
3. Do not use complete rest as a treatment strategy
Rest reduces pain in the short term by removing the provocative load — but it also reduces tendon capacity, setting up a reactive spike when you return to activity. The goal is to find a level of loading that keeps the tendon working without exceeding its current threshold, while the rehabilitation programme progressively raises that threshold.
4. Review your training load history
Patellar tendinopathy rarely appears without a preceding period of load spike — a sudden increase in volume, a return to heavy training after a break, or the accumulation of a competition season without adequate recovery. Identifying the load event that triggered the condition helps to avoid repeating it once the tendon has recovered.
Take the Next Step
Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
📄 Free 2-Week Rehab Program — request your copy
Frequently Asked Questions
References
- PubMed Malliaras P, Cook J, Purdam C, Rio E (2015). Patellar tendinopathy: clinical diagnosis, load management, and advice for challenging case presentations. Journal of Orthopaedic & Sports Physical Therapy, 45(11), 887–898.
- PubMed Cook JL, Purdam CR (2009). Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. British Journal of Sports Medicine, 43(6), 409–416.
- PubMed Powers CM (2010). The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 42–51.
- PubMed Arumugam A, Harikesavan K (2021). Effectiveness of fascial manipulation on pain and disability in musculoskeletal conditions: a systematic review. Journal of Bodywork and Movement Therapies, 25, 100–109.