Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
What Is ITB Syndrome?
The iliotibial band — more accurately described as the iliotibial tract (ITT) — is not a discrete anatomical band. It is the lateral condensation of the deep fascia of the thigh: a longitudinal thickening of the fascia lata that runs from the iliac crest to the lateral tibia, with broad fascial attachments to the lateral intermuscular septum, the greater trochanter, and — critically — an oblique expansion passing under the lateral patella into the anterior knee retinaculum. It is, in Carla Stecco's framing, part of the fascial stocking of the thigh that coordinates the actions of the gluteus maximus and vastus lateralis through a shared fascial environment.
ITB syndrome is lateral knee pain arising from overload of this structure, most commonly in runners and cyclists. It accounts for approximately 10% of all running-related injuries and is among the most common causes of lateral knee pain in endurance athletes.
The mechanism is compression, not friction
For decades, ITB syndrome was explained as the band repeatedly sliding anteriorly over the lateral femoral epicondyle during knee flexion — "friction syndrome." Cadaveric, MRI, and histological studies have directly challenged this model. The ITB is firmly anchored to the distal femur by fibrous strands and cannot translate anteroposteriorly — it is part of the fascia lata, not a free-moving structure. What appears to be movement is an illusion created by sequential tension shifting between the anterior and posterior fibres of the tract as the knee moves through flexion [131].
What the research does show is that the ITB is compressed against the lateral epicondyle at approximately 30° of knee flexion — the angle at which the foot strikes the ground during running. Beneath the ITB at this point is a layer of richly innervated fat containing Pacinian corpuscles. No bursa was found in any cadaveric or imaging study. The pain in ITB syndrome arises from compression of this innervated fat pad, not from friction on the lateral condyle [131]. This distinction matters clinically: treatment aimed at reducing ITB "friction" misses the target.
Presentation overview
| Feature | Detail |
|---|---|
| Pain location | Lateral knee; over lateral femoral epicondyle; sometimes distal ITT or lateral hip |
| Symptom pattern | Onset at predictable running distance or time; may be sharp or burning; eases with rest |
| Provocative activities | Running (especially downhill), cycling, repeated knee flexion/extension under load |
| Critical angle | Pain typically at ~30° knee flexion — the compression zone |
| Noble compression test | Pain with pressure over lateral epicondyle at ~30° flexion |
| Most affected | Distance runners, cyclists, military personnel; rapid mileage increases |
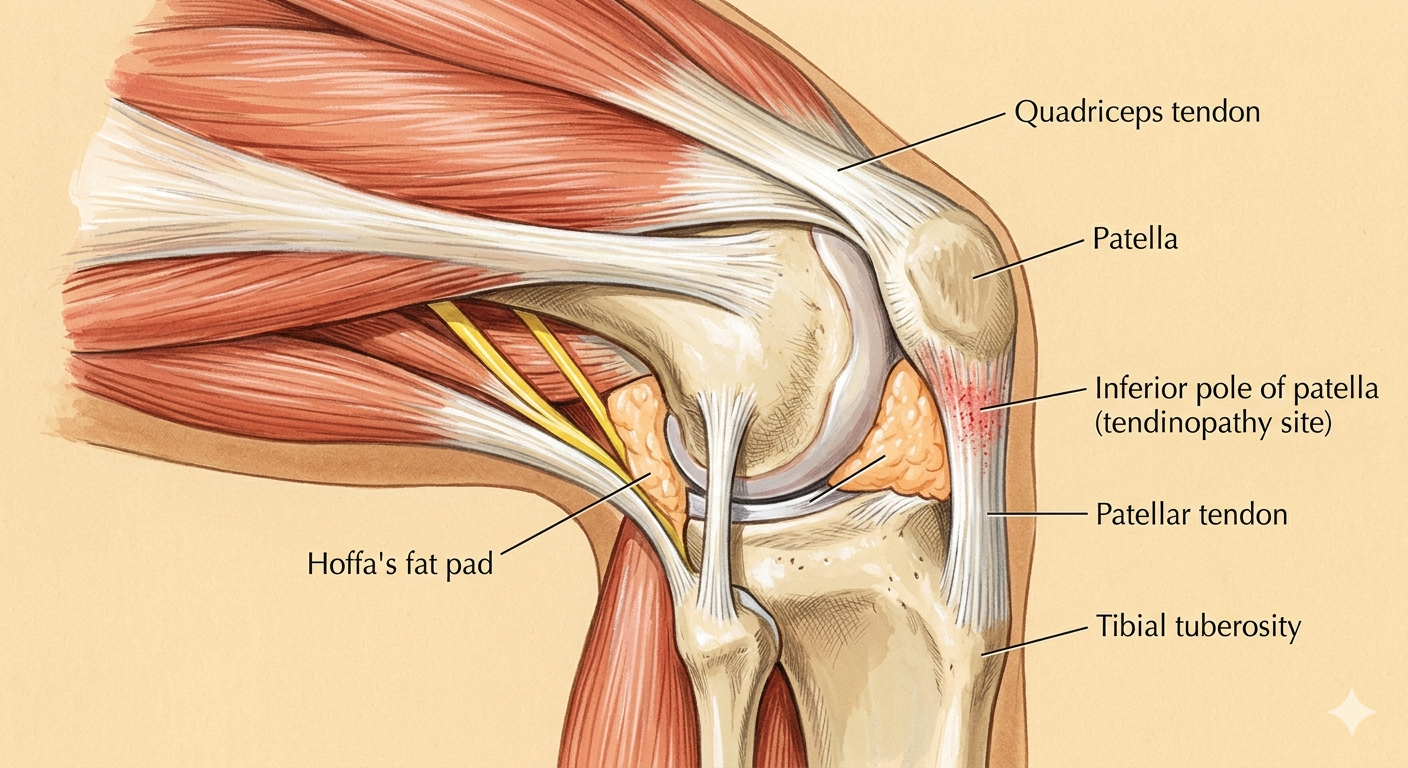
The knee joint — patella, patellar tendon, femoral condyles, and tibial plateau. The relationship between these structures, and the forces transmitted through them during movement, determines how load is distributed across the joint.
Who Typically Experiences This?
The runner who has increased their mileage
A sudden increase in running volume is the most consistent risk factor for ITB syndrome. The combination of increased total load on the lateral fascial system and the cumulative fatigue-related decline in hip abductor function — which occurs progressively through longer runs — creates the conditions for overload. In clinical practice, ITB syndrome often presents in runners who have recently pushed through a distance milestone or ramped up training for an event.
The cyclist with bike fit issues
In cyclists, ITB syndrome typically relates to saddle height. A saddle set too high results in excessive hip drop and pelvic tilt on the downstroke, which increases the valgus stress through the lateral knee. A saddle set too low keeps the knee in deeper flexion through the pedal stroke, increasing the duration of ITB compression at the lateral epicondyle. Either pattern, sustained through thousands of pedal revolutions, is a recognised driver of lateral knee pain in cyclists.
The runner with weak hip abductors
Hip abductor weakness is the most consistently documented intrinsic risk factor for ITB syndrome. Research found that hip abductor strength was 20–18% below controls in runners with ITBS. Critically, following six weeks of targeted hip abductor strengthening, 92% of runners with this presentation returned to pain-free running [132]. The hip is not a secondary consideration in this condition — it is often the primary driver.
The person returning from injury or extended rest
After a period of deconditioning — injury, illness, or a training break — the hip abductors and posterior chain are relatively underloaded. Returning to full running volume without a corresponding period of hip strengthening leaves the lateral knee fascial system absorbing load without adequate proximal support. This is one of the most common presentations in recreational runners who return to training "too fast, too soon."
The trail runner or military recruit
Downhill running increases the knee flexion angle at foot strike, keeping the knee in the ITB compression zone for longer. Trail runners and military personnel doing repeated hill training are particularly susceptible, as are those training on cambered surfaces where one leg is consistently loaded in more valgus than the other.
The Fascial Lens: Why We See This Differently
The ITB is a fascial structure, not a band
The conventional view of the ITB as a discrete band that can be "stretched" or "rolled out" misunderstands its anatomy. The ITT is a thickening of the fascia lata — the deep fascial stocking of the thigh. It is extensively connected to the lateral intermuscular septum and anchored to the distal femur; it cannot be meaningfully stretched or elongated in isolation, because it is part of the thigh's fascial architecture [131].
This is why foam rolling the lateral thigh does not elongate the ITB. What it may do is change the mechanical properties of the loose connective tissue within the deeper fascial layers — reducing densification and restoring gliding capacity between fascial planes. Research provides preliminary evidence that myofascial release adds measurable benefit to hip strengthening in ITBS: an RCT found that MFR combined with hip strengthening produced significantly greater ITB thickness reduction on ultrasound at four weeks (mean difference −0.66mm, p=0.013) and faster pain relief at two weeks compared to strengthening alone [135]. The structural finding — reduced ITB thickness — suggests the MFR is affecting the tissue, not merely the pain experience.
The deep longitudinal sling connects the ITB from below
The biceps femoris is a component of the deep longitudinal sling — the posterior chain connecting the lumbar spine through the sacrotuberous ligament to the biceps femoris and, through the leg, to the peroneal chain. The biceps femoris inserts into the head of the fibula and has fascial continuity with the lateral lower leg. The proximal biceps femoris also has connections to the posterior ITT. When the DLS is restricted — through hamstring densification, STL restriction, or poor lumbopelvic load transfer — the lateral thigh fascial system is loaded from below, contributing to the environment of lateral knee overload.
Hip mechanics determine how much compression force reaches the fat pad
Poor hip abductor control during running allows the pelvis to drop on the swing side — the Trendelenburg pattern. The stance limb compensates with increased hip adduction, directing the knee joint centre medially. This increases the valgus force through the knee and places the ITB under greater tension. At the same moment, the ITB is being compressed against the lateral epicondyle by the 30° flexion angle of foot strike. The combination of increased tension and cyclical compression, sustained over thousands of strides, is the mechanical loading pattern that drives the condition [132].
Hip abduction weakness is 20% below controls in runners with ITBS. Addressing this is not an adjunct to treatment — it is the primary intervention that addresses the mechanical driver [132].
Densification of the lateral thigh fascial system
The IT tract and the deep fascia of the lateral thigh are subject to the same densification process seen throughout the body's fascial system: progressive thickening of the loose connective tissue between fascial layers, with increased hyaluronan viscosity impairing gliding. In ITBS, this densification develops in response to sustained compressive and tensile load. It reduces the capacity of the lateral thigh fascial system to distribute load efficiently, concentrating mechanical stress at the compression point over the lateral epicondyle. Restoring normal fascial gliding in this system — through FM directed at the relevant centres of coordination in the lateral thigh and hip — is a component of how we approach this condition.
What Does the Research Say?
ITB syndrome is a compression problem, not a friction problem
Cadaveric, histological, and MRI studies confirmed that the ITB is anchored to the distal femur and does not slide anteroposteriorly over the lateral epicondyle. Pain arises from compression of a richly innervated fat pad deep to the ITB at approximately 30° of knee flexion. No bursa was identified in any specimen. This reframes the pathomechanism and the treatment target — compression reduction and load management, not ITB stretching or friction reduction [131].
Hip abductor weakness is a primary driver — and a treatment target
Evidence documents that hip abductor strength is consistently 18–20% below controls in runners with ITBS. Importantly, after six weeks of targeted hip abductor strengthening, 92% of runners with ITBS returned to pain-free running — underscoring the causal relevance of hip abductor control rather than local knee treatment [132].
Hip mechanics determine lateral knee load
A clinical commentary on hip mechanics and knee injury established that hip adduction is the primary contributor to dynamic knee valgus, which increases tension in the lateral fascial system including the IT tract. Poor proximal control of hip adduction and internal rotation directly increases the compressive and tensile load on the lateral knee with every stride [132].
Myofascial release accelerates recovery and reduces ITB thickness
A randomised controlled trial found that myofascial release combined with hip strengthening produced significantly greater ITB thickness reduction on ultrasound at four weeks (mean difference −0.66mm, p=0.013, large effect) and significantly faster pain reduction at two weeks compared to hip strengthening alone. This is the first RCT demonstrating structural fascial change (ITB thickness reduction) through MFR in ITBS [135].
Fascial manipulation — effectiveness across MSK conditions
A systematic review of fascial manipulation across musculoskeletal conditions found evidence supporting its effectiveness for pain and disability in MSK presentations [19]. Fascial approaches directed at the lateral thigh fascial system and the proximal hip chain complement the hip rehabilitation programme.
How We Approach ITB Syndrome
Load assessment and biomechanical analysis
Our assessment begins with running or activity pattern analysis — identifying the load that is provoking the condition and understanding the volume, terrain, and footwear context. We assess the single-leg squat and running gait (where available) for dynamic knee valgus and Trendelenburg pattern, as indicators of the proximal driver. We also assess hip abductor and external rotator strength bilaterally and lumbopelvic stability in single-leg stance.
Fascial Manipulation assessment
We assess the lateral thigh fascial system — the iliotibial tract, lateral intermuscular septum, and biceps femoris — for centres of coordination where densification may be contributing to the lateral knee compression environment. Using the Stecco FM approach, treatment at these points aims to restore normal fascial gliding in the lateral thigh system and reduce the tension load on the sub-ITB fat pad [19, 135].
Hip abductor and posterior chain rehabilitation
Consistent with the evidence, we prioritise hip abductor and gluteus maximus strengthening as the primary rehabilitation intervention — addressing the proximal driver of increased lateral knee compressive load [132]. We progress from isolated hip abductor and external rotation work to integrated single-leg and running-specific loading.
Load management and return to running
We work with runners to manage volume and intensity while rehabilitation progresses — maintaining aerobic fitness through lower-risk activities (pool running, cycling on a well-fitted bike) while reducing the specific compressive loading pattern. Return to running is graduated, with attention to pace, terrain, and stride mechanics.
New to Fascial Manipulation? Read how it works →
Please note: The information on this page describes our general clinical approach and is intended for educational purposes only. Individual presentations vary, and your assessment and management will be tailored specifically to you. Nothing on this page constitutes clinical advice for your individual situation. Please consult a registered health practitioner for advice about your specific condition.
What Can You Do Right Now?
1. Stop foam rolling the lateral thigh as a treatment
Foam rolling the IT tract does not elongate or "loosen" the ITB — the anatomy does not allow this. If foam rolling provides temporary relief, it is likely through the nervous system rather than mechanical elongation of the tract. The underlying mechanical driver — hip abductor insufficiency — is not addressed by foam rolling, and relying on it delays the rehabilitation that will actually change the pattern.
2. Start hip abductor work immediately
Side-lying hip abduction, clamshells, banded walks, and single-leg bridges directly target the gluteus medius and gluteus maximus — the muscles whose insufficiency drives the lateral knee overload pattern. The research is clear: 92% of runners returned to pain-free running after six weeks of hip abductor strengthening [132]. This is the most evidence-supported self-management step available.
3. Temporarily reduce your running volume
While the hip strengthening programme is in its early stages, temporarily reducing running volume — and avoiding downhill running — reduces the compressive load on the lateral knee. This is not indefinite rest; it is short-term load reduction to allow the irritated fat pad to settle while the proximal rehabilitation begins.
4. Review your bike fit if you cycle
If cycling is also provocative, a saddle height check is worthwhile. The lateral knee compression that drives ITB syndrome in cyclists is closely related to saddle position. A simple assessment by a bike fitter familiar with overuse injury can often identify and correct the contributing factor quickly.
Take the Next Step
Ready to get on top of this?
📞 Call Now — speak with our team
🗓 Book Online — available 24/7
Frequently Asked Questions
References
- PubMed Fairclough J, Hayashi K, Toumi H, et al. (2006). The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. Journal of Anatomy, 208(3), 309–316.
- PubMed Powers CM (2010). The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 42–51.
- PubMed Ming Z, Dong G, Luo L, Yuan L, Li Y (2025). The combined effect of myofascial release and hip strength training on iliotibial band syndrome: a preliminary randomized controlled trial. Complementary Therapies in Medicine, 95, 103274.
- PubMed Arumugam A, Harikesavan K (2021). Effectiveness of fascial manipulation on pain and disability in musculoskeletal conditions: a systematic review. Journal of Bodywork and Movement Therapies, 25, 100–109.